He has a history of joint surgery because of trauma, and prothesis, dating 4 years before.
He is HIV positive
He presents feverish (38°C), the left knee is swollen and hot.
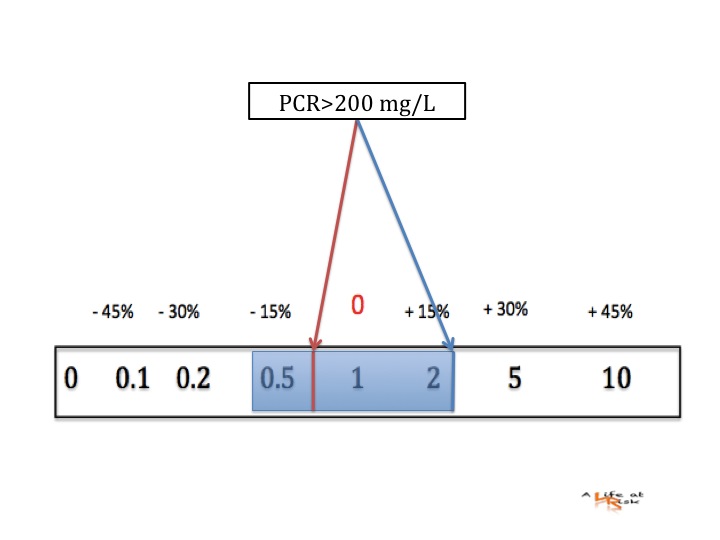
WBC 34.000/μL, CRP 109 mg/L, PCT 0,05 ng/mL.
As we have seen in previous post, history, clinical examination and serum test are not useful to rule out or in a septic arthritis. It’s time to perform arthrocentesis: sWBC: 60x109, sLactate: 10 mmol/L
Are this findings useful?



Conclusion
Although arthrocentesis is not a risk-free procedure, synovial fluid analysis is essential for the diagnosis.
sWBC count has been studied in several trials but a significant heterogeneity was noted so it should not be used in isolation to rule in or rule out the diagnosis of septic arthritis, anyway it should augment the entire clinical evaluation.
Synovial lactate, instead, has consistently demonstrated desirable diagnostic properties to rule in septic arthritis using a threshold of >10 mmol ⁄ L.
Bibliography
C. R. Carpenter et al;
Evidence-based Diagnostics: Adult Septic Arthritis
Acad Emerg Med Aug 2011, vol 18 n 8.
Read more...